


The Tennessee shooting and the avalanche of medicated shooters headed to our schools
Brain injury and trauma, Ritalin and Adderall, Xanax and SSRIs, dysphoria and disembodiment


This post will exceed the limit of what your email providers allow to be sent to your inbox. Please click through on the headline to read the entire piece.
Evelyn Dieckhaus, 9 years old. William Kinney, 9 years old. Hallie Scruggs, 9 years old and the daughter of the church’s senior pastor. Mike Hill, 61 and the school’s custodian. Cynthia Peak, 61 and a substitute teacher. Katherine Koonce, 60, the school’s headmaster, who died in the middle of the hallway, running straight towards the shooter. They were children, daughters, sons, sisters, brothers, spouses, parents, and grandparents. They were each so special to so many.
At 10:10 Monday morning, a 28-year-old woman named Audrey Hale shot open the glass door of The Covenant School, a Nashville Christian school we’re told she attended as a child. Hale made her entry to the classrooms and killed these precious children and their caretakers before two heroic Nashville police officers, Rex Engelbert and Michael Collazo, took her down. Every parent’s worst nightmare happened. Again.
I cannot fathom the tidal wave of shock and horror the families of those killed in Tennessee suddenly found themselves thrown into. I cannot imagine how they all sat up through the night, crying and praying, asking questions no one will ever have the answers for. My heart breaks at the thought of them finally falling asleep at four in the morning, only to awaken a few hours later and remember it all over again. May the Lord bring these families peace in knowing their children are wrapped in the love of God. I pray that they made their swift exits before ever having the chance to feel an ounce of fear or a moment of suffering. May the surviving teachers and children who witnessed this horrific act be soothed by their families and unconditionally supported by their community. And may something good come from this tragedy. For a few moments, hold their names in your heart.
If you feel called to do so, you can donate to the families of the victims through the Community Foundation of Middle Tennessee. All donations, less credit card fees, will go to the families.
A Rare Female Shooter
When I heard that the Tennessee school shooter was female, I knew instantly this would be no ordinary female. I knew without looking further that the shooter was a heavily medicated biological female identifying as transgender with high functioning autism. I knew this beyond all doubt because I’ve researched school shootings and pharma meds before. Females almost never take up guns against others, and unmedicated females simply do not shoot up schools. Ever.
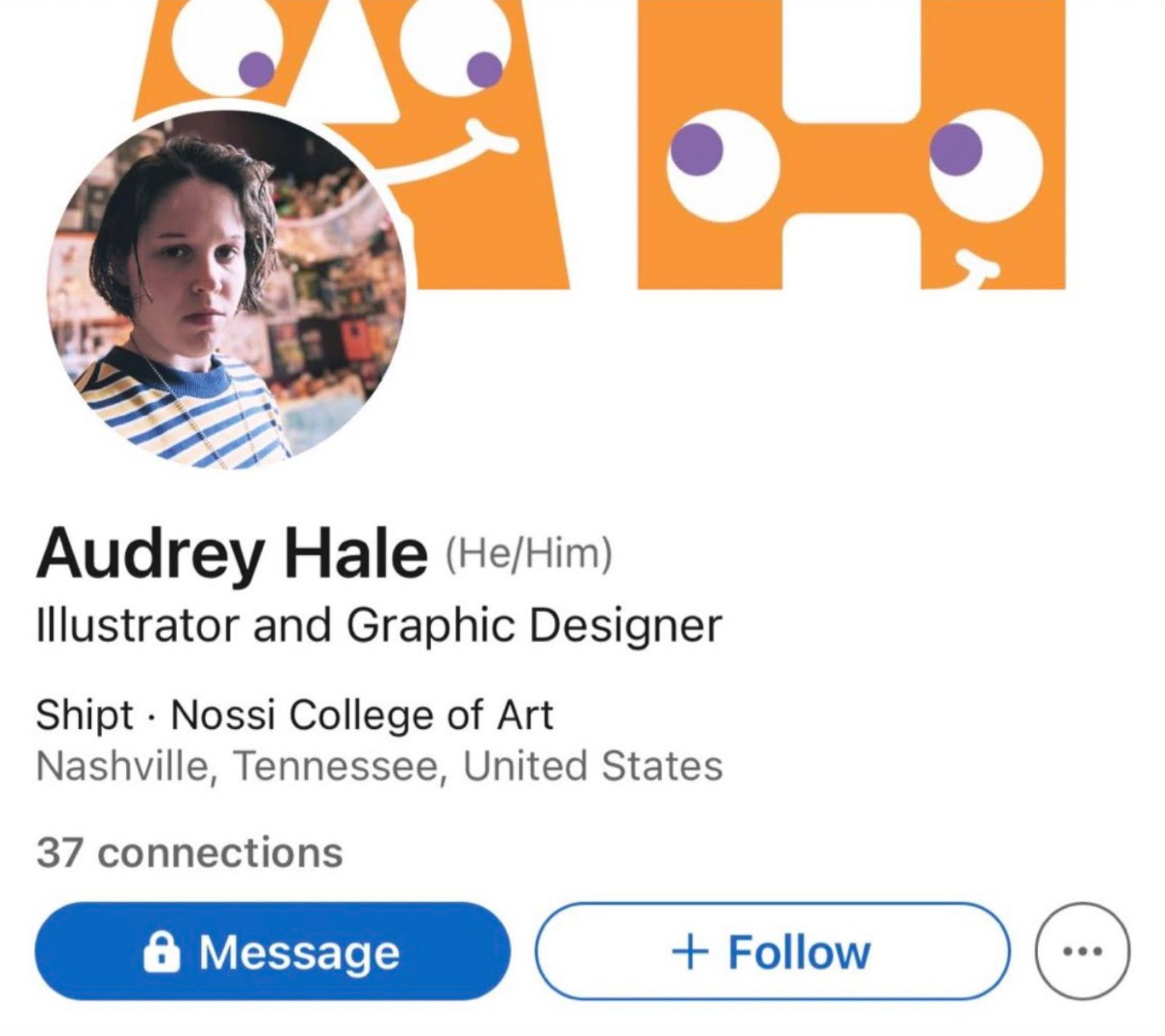
Sure enough, I waited a bit and there they were: the cross-sex pronouns. Later that night, a source close to the Hale family told the Daily Beast that Hale was a “high-functioning autistic under a doctor’s care.”
America, we are in crisis. And despite how abhorrent you or I may find them, I’m not talking about drag queens, male prostitutes, pedophiles, or the men with brazen sexual fetishes that we’re all forced to publicly deal with now. I’m not talking about rapists who declare themselves to be transgender to get housed with female inmates so they can keep on raping. I’m talking about our well-loved and cared for children and young adults in crisis.
Every single one of our kids and young adults deserves love, without exception. They deserve help; they deserve supportive treatment that doesn’t involve having prescriptions thrown at them as the only solution or even one solution of many. In fact, they deserve to be sheltered from predatory pediatricians, psychiatrists, and surgeons entirely as they weather this storm. The first steps taken when someone expresses that they’re experiencing gender dysphoria should be to get them off social media at all costs, remove them from the dysphoric influences, and keep them far away from doctors.
Quite immediately after the Tennessee shooting, Snopes was on the case to get to the bottom of whether Audrey Hale was the first female school shooter. Whenever reading about this shooter, notice how writers sometimes conflate her, a person who identified as being “trans,” with “other mass shooters” to muddy the waters of what we’re talking about so that they can say, “99% of mass shooters aren’t gay, non-binary or trans.” I’m not talking about all mass shooters, but, I’m telling you, with love and compassion and respect for all human beings who are hurting, if you look into the number of school shooters in the last 24 years who were gay, bullied by classmates for allegedly being gay, non-binary or trans, you’ll start to wonder if there is a media conspiracy to keep the public from knowing about the alleged sexual orientations of recent school shooters. The fact that CBS news execs were caught red handed contorting themselves into pretzels to avoid saying that Audrey Hale was female identifying as a transgender male bolsters my point.
I want to be crystal clear: a gay kid or one who thinks they’re trans isn’t the threat to school safety. As I said years ago, it’s the kids prescribed antidepressants, anti-anxiety, and ADHD drugs who are the threat to school safety. It has always been those kids and it always will be.
In their answer on the subject of female shooters, Snopes found it necessary to reach all the way back to Brenda Spencer in 1979. I covered Brenda Spencer when I wrote about school shooters years ago. At the time, she was a 16-year-old drug and alcohol abuser who relayed to some people that she was a victim of physical violence and incest. Friends who knew her described her in ways that convey that she appeared outwardly to suffer from hallucinations and delusions of grandeur.

For reasons known only to Snopes, their reporter skipped right past the May 7, 2019, shooting at STEM School in Highlands Ranch, Colorado, where the star of the robotics team was murdered, and eight other kids injured. I remember that once the scrawny, 95-pound fuchsia-haired Devon Erickson, an 18-year-old “edgy” male who loved to perform musical theater, was photographed at his arraignment, the story was dropped from mainstream media like a hot potato. By the time it came out that his previously-described-as-male accomplice, 16-year-old Alec McKinney, who was female but used male pronouns, had plotted the school shooting as revenge on classmates over bullying, media coverage was almost non-existent. McKinney told friends that her mom wouldn’t approve for her to take testosterone, she was an avid coke and Xanax abuser, and a self-harm cutter. She told the police she wanted her classmates “to have to suffer from trauma like she has had to.”
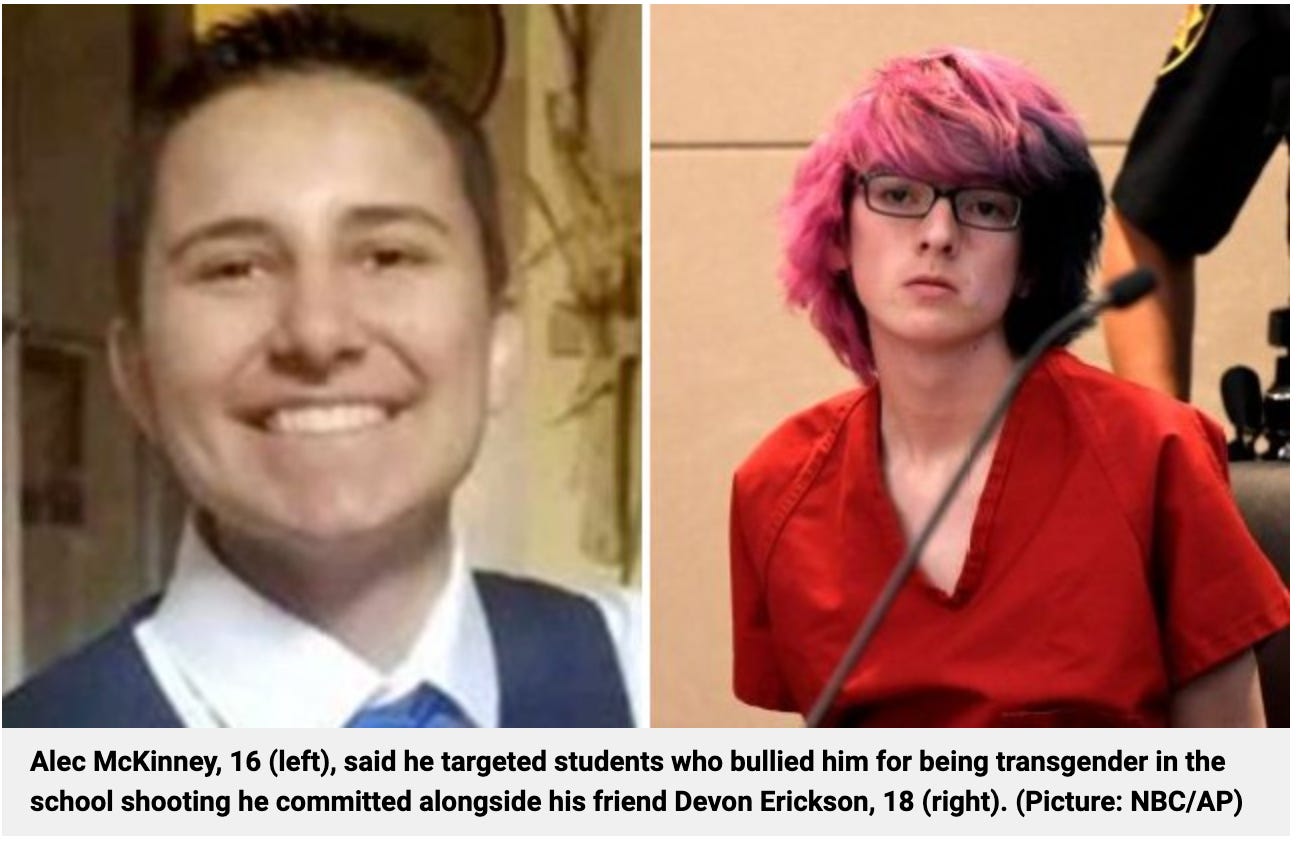
By the time of a key November 2019 disclosure from McKinney’s psychiatric nurse practitioner, the media was long gone. The nurse testified that he prescribed McKinney ADHD medication to take “along with” the antidepressants and mood stabilizers she was already taking. I only found these details covered in the Denver Post, and the Post reporter thought the prescription drug information was best presented buried 16 paragraphs deep in his 19 paragraph story.
Someone please show me the scientific studies that investigate the consequences of kids popping 20 milligrams of Prozac for depression and another 60 milligrams of Adderall for their so-called ADHD, Klonopin or Xanax for anxiety and OCD behaviors and a bit of pharmaceutical grade lithium for mood stabilizing. How in the world is psychiatry still a condoned medical practice? Tom Cruise hit the nail on the head 18 years ago, you’ll never change my mind.
What are we allowing to happen to these children? McKinney was on at least three powerful, mind-altering psychotropic prescriptions at 16-years-old? And now, in many cases, we’re adding testosterone to the mix, often without parental knowledge or consent.
Dissociation from One’s Own Body
Dissociative disorders are described as an involuntary escape from reality characterized by a disconnection between thoughts, identity, consciousness and memory. Kids suffering from dissociative disorders experience detachment or depersonalization, which is feeling as if they are outside of their own body, as well as loss of memory or amnesia. Dissociative disorders can happen when kids have lived through traumatic events—and the events they lived through don’t need to be traumatic to me or you, to a judge or jury, or to the general public. Just traumatic to them. Taking Xanax for anxiety can also cause depersonalization. It also causes derealization, where they have a sense that things around them aren’t real. Ritalin causes people to feel nervous and irritable. Aderrall causes users to become disconnected from the feelings of others, as well as increases irritability and aggression. Do you know what testosterone therapy does? It increases aggression significantly. Does this sound like a pharmaceutical recipe for school shooters?
If you go looking for peer-reviewed journal articles that prove the link between antidepressants and school shooters, you aren’t going to find one. Proving that link is just as popular as researchers getting millions of dollars to prove vaccines are injuring our kids. Remember when Dr. Kelly Brogan earned the largest book advance in the history of Harper Collins to write A Mind of Your Own, a book about the dangers of antidepressants and how to taper off? Then she couldn’t get one single mainstream media interview to support the book because pharma owns the media. She had to quickly pivot to a grassroots social media campaign to successfully land herself on the New York Times Bestseller list.
Confounding the issue is the fact that people who tally school shootings muddy the waters to keep the obvious hidden. Under all “school shooter” trackers we find gang fights, accidental gun discharges, drive bys, disgruntled adult employees, and shots fired on school property that aren't related to a student bringing a gun to school to kill people, such as college parties. I think I speak for most parents when I say I am most concerned about the student or former student who brings a gun into a school during school hours, when students are present, with the intent to kill. I have yet to find that list.
However, what you can find, are the peer-reviewed articles that link antidepressant use to hypomania—a state of over-active and high energy behavior that is a milder version of mania, which is quite likely the mental state these medicated kids and young adults are in when they commit suicide, homicide, or shoot up a school. This state of hypomania doesn’t affect all kids or even the majority of kids. It seems to impact the kids who are actually bipolar, and who should never have been given antidepressants in the first place.
From the conclusion of a 1987 study: “We believe that the available evidence suggests that antidepressants can precipitate mania and hypomania in bipolar patients." "Of more practical interest is the question of whether the combination of lithium and antidepressants is associated with a higher rate of manic switches than lithium alone."
A 2003 review: “About one-quarter to one-third of bipolar patients may be inherently susceptible to antidepressant-induced manias. Bipolar patients with a strong genetic loading for bipolar illness whose initial illness begins in adolescence or young adulthood may be especially at risk. Further efforts are needed to better identify high-vulnerability subgroups and differentiate illness-specific from medication-specific factors in mood destabilization."
A 2005 study: "Children, adolescents, and young adults treated for depressive or anxiety disorders showed an increased risk of new-onset mania at ages 15 to 25 years.”
A 2012 review: “SSRIs may be particularly problematic in specific populations, such as those with some symptoms of mania or a family history of Bipolar Disorder (BD), but the precise risk is unknown. There is no clear evidence that stimulants or SSRIs accelerate the natural course of BD development in overall samples, but in individual cases prescribers should proceed cautiously when using these agents in youth already at risk for developing BD, such as those with ADHD and mood dysregulation, a history of prior AIM, a history of psychosis, or a family history of BD.”
Body Identity
Let’s look at two other identity disorders similar to gender dysphoria. You’ve probably heard of Body Dysmorphic Disorder, where people misperceive defects in their appearance, such as viewing themselves as being grossly overweight when, in reality, they’re desperately underweight. While BDD can be caused by trauma, it’s known that there are observable, physical traits in the brains of people who suffer from it.

Secondly, have you heard of Body Integrity Identity Disorder? It’s where people are overcome with desire to amputate one or more healthy limbs or cut their spinal cords because they want to be paralyzed. Beginning in childhood, these people internally view themselves as a paralyzed person despite not being paralyzed at all; some people suffering from it even use wheelchairs all day despite being completely able-bodied. They feel there is a mismatch between their actual body and their perceived body, so they go from doctor to doctor trying to get spinal cord transection surgery or amputations because they don’t want to feel sensation in the limbs they don’t think are supposed to be there. Some people end up self-amputating, and some of them find corrupt doctors to perform the surgery. A 2017 survey of 80 people suffering from BIID found that respondents were motivated to amputate a body part in order to “restore their identity,” does that sound familiar? 57 of the 80 respondents admitted that their desire for the amputation accompanied feelings and cognitions of sexual arousal, and 38 of the 57 admitted that this sexual arousal was an additional motivator for wanting to amputate a limb or paralyze themselves. While the authors didn’t give the numbers in the abstract, they noted that the “people in the sexually aroused group were significantly more likely to be homosexual men.”
But look at this: “Neurological results suggest that BIID is a brain disorder producing a disruption of the body image, for which parallels for stroke patients are known.” And, “The symptoms of BIID parallel those in somatoparaphrenia (when paralyzed people feel like their paralyzed limb doesn’t belong to them), a syndrome occurring secondary to right parietal lobe damage by a cerebral tumor or stroke.”
Does your stomach turn in knots at the thought of an unethical doctor willing to take a payday in exchange for cutting a spinal cord or amputating someone’s healthy leg to feed a mental disorder caused by what might be a brain injury caused by something similar to a stroke? Yet 27% of Americans believe insurance companies should pay out to amputate a dysphoric boy’s penis or a girl’s breasts. Many gender dysphoric girls decline have their nipples sewn back on after undergoing a double mastectomy because it helps them feel more non-binary or, in some cases, they prefer the esthetic of looking less human without them. How far away are we from allowing people suffering from BIID to cut off their arms and legs upon request with a supporting psychiatrist note? Not far, friends. A 2012 article on BIID argued that amputation results in an “impressive improvement in the quality of life” for people suffering from BIID, and “respect for their desires is an important first step in providing them care.” A BIID “Day of Visibility” is on the horizon.
Gender dysphoric people are, obviously, already feeling disassociated from their bodies, and they have a high prevalence of dissociative disorder of any kind. While we don’t entirely understand what causes dissociation, these kids need help. They need embodiment work, they need movement, they need connection to themselves—their real selves, not affirmation of the dark depths of their imagination. They probably need a DMSA-provoked heavy metals test and a supervised chelation plan. Enrollment in a program like Brain Balance would be beneficial. Most importantly, they need time. Some of them need services to process horrific traumas—which can impact both the function and structure of the amygdala, hippocampus, and prefrontal cortex of their brains.

In December 2021, New York Magazine ran an article about a female Mother Jones civil rights reporter, Mac McClelland, who transitioned to male as an adult. What the article failed to mention, however, is that, many years prior, McClelland was witness to sexual violence while working in Burma, the Democratic Republic of Congo, and Haiti. After meeting a rape victim, taking the victim to the hospital and seeing how she was discarded as worthless, McClelland became so traumatized that she convinced herself that the only cure to her trauma was to endure a violent rape herself, so she staged one—with herself as the victim. Still, nine years later, she cut off her breasts, removed her uterus, and had a fake penis made from the skin of her thigh at the age of 39. Given her history and unorthodox rape therapy, who signed off on this?
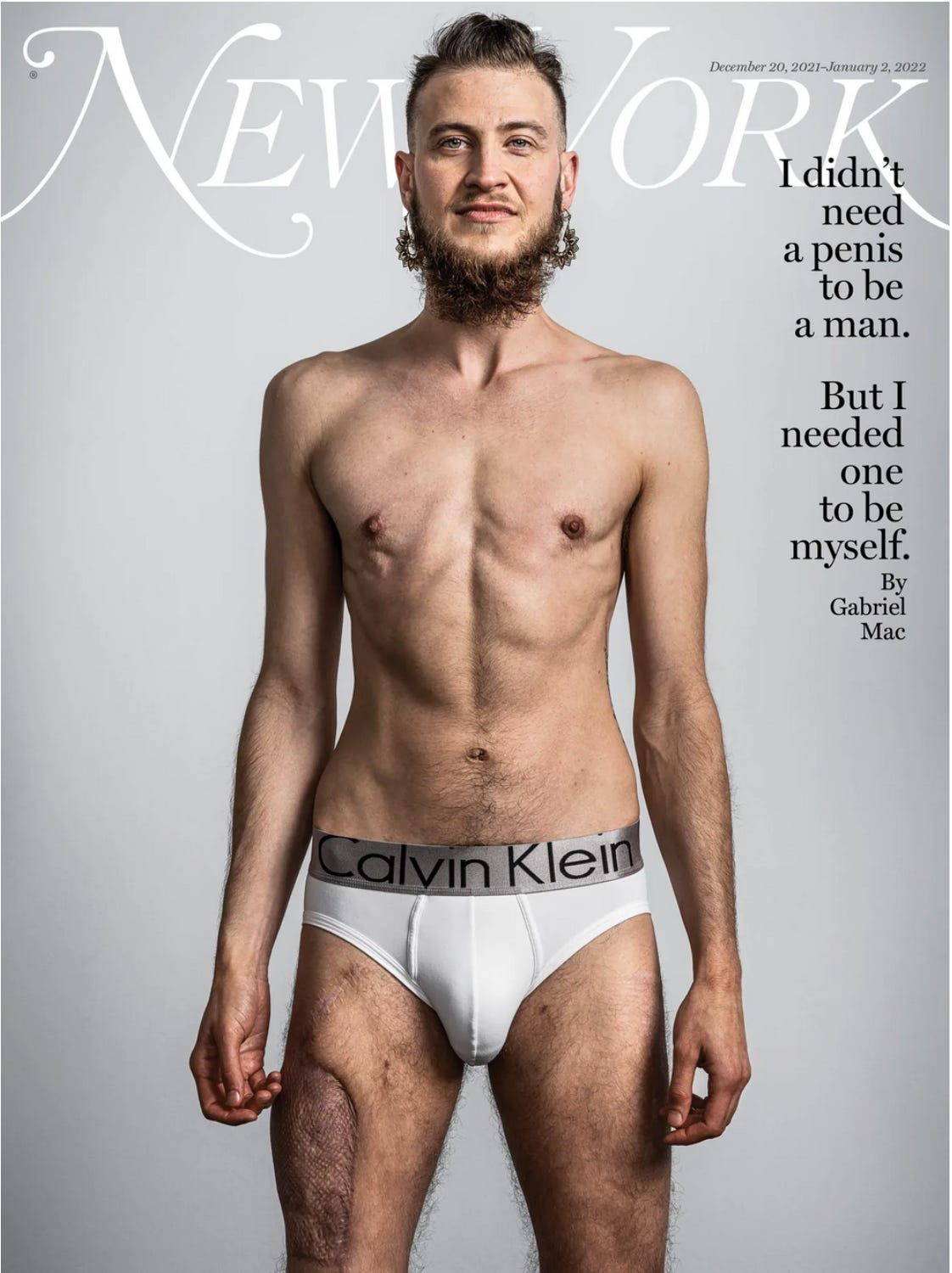
Friends. I shouldn’t have to say this, but surgery is not helping anyone. Cutting a pretend penis out of a woman’s thigh is not a solution to any trauma. It doesn’t make anyone less suicidal. My heart hurts for these people.
As the pendulum has swung too far too fast, formerly-trans-identifying kids are starting to fight back. 18-year-old Chloe Cole, a female allowed to take cross-sex hormones at age 13—hormones that damaged her for life—just sued Kaiser in February for allowing surgeons to railroad her into a “mutilating sex change experiment” as a minor.
Tidal waves of these lawsuits are coming. If you know someone struggling with gender dysphoria, or the issue is in their family, I have a few resources for you. Genspect is a non-partisan, independent organization advocating for a neutral approach to this rising epidemic. They have gay and lesbian members on their team. Partners for Ethical Care is another non-partisan grassroots group. Parents of ROGD Kids for parents of kids experiencing rapid-onset gender dysphoria that may be more related to recent trauma or social contagion. The one-woman force behind Whose Body Is It has a free resource guide you can get with an email signup.
The Autism and Transgender Overlap
I’m not going to argue that there’s only one way into transgenderism any more than I’d argue there’s only one way into autism. But just like autism, the overwhelming majority of cases have one driving force. And we have a clue that it’s the same driving force as autism because of the glaring overlap between high functioning autism and gender dysphoria.
Anecdotally, there also seems to be a social contagion aspect to rapid-onset gender dysphoria in some teen girls, especially when three or four close friends are found to have begun visiting gender clinics in quick succession. While it’s possible these girls are suffering from social contagion, it’s also possible some, if not all, have undiagnosed high functioning autism. What used to be called “Asperger’s Syndrome” is notoriously missed in girls because it presents differently than in boys, and the entire diagnosis has been built around boys. Girls with Asperger’s Syndrome have social development more on par with typical boys; that is to say well above high-functioning autistic boys but not on the level of typical girls. They may be overly emotionally sensitive, intense, overwhelmed by crowds, bothered by food or fabric textures, and socially awkward. They struggle to form typical intimate female friendships and often miss out on the meaning of sarcastic comments. They may have an overlapping diagnosis with OCD or anorexia. But these girls are good at mimicking the behavior of girls around them and incorporate female behaviors they see in movies or read in books into their own, which, in the context of “social contagion mimicry,” lends itself to the idea that there likely is a lot of undiagnosed high functioning autism in females suddenly experiencing gender dysphoria in clusters.
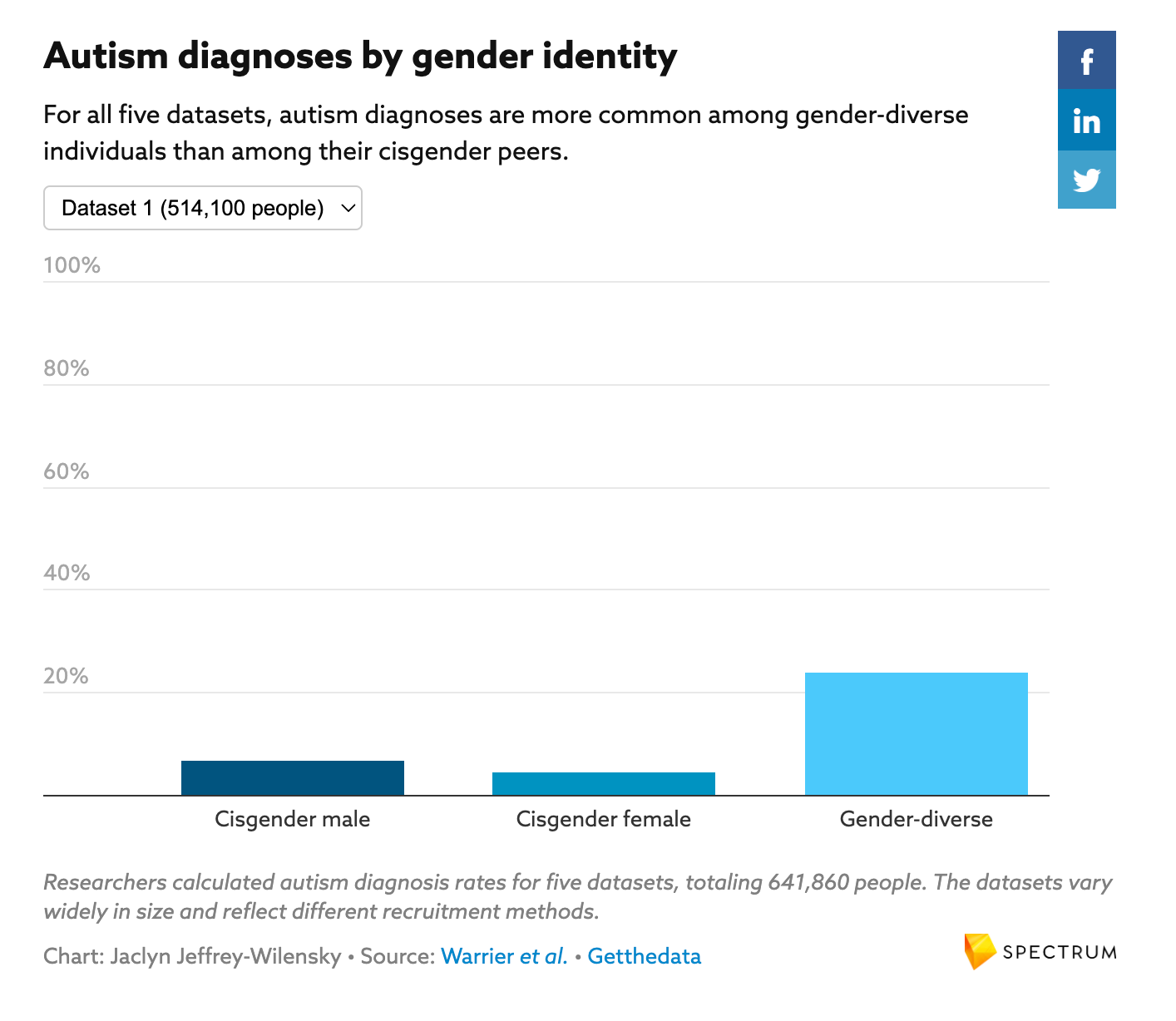
One dataset I found (entitled “Elevated rates of autism, other neurodevelopmental and psychiatric diagnoses, and autistic traits in transgender and gender-diverse individuals,” Varun Warrier, 2020) showed that in a study of 514,100 kids, 7% of boys and 4% of girls who were not gender dysphoric were diagnosed as being under the autism umbrella. Yet, 24% of gender dysphoric kids have a (high functioning) autism diagnosis. Kids are are more than twice as likely to have an autism diagnosis if they also suffer from gender dysphoria. Where are the alarms?
Do you all remember how, for so many years, the ladies of the Thinking Moms’ Revolution screamed from the rooftops that autism isn’t a mental disorder, it’s a medical condition?
My belief is that so is the gender dysphoria seen in autistic people. It’s a medical condition related to the brain injury that resulted in their autistic symptoms.
To be fair, I do know of a couple of non-vax kids with gender dysphoria but I also know a couple of non-vax kids with deadly peanut allergies and a couple more with classic autism—only because I happen to know a lot of people in the movement. Just because I know two of each doesn’t mean I’m obligated to engage in false equivalency and pretend that vaccination and brain injury, from both aluminum damage and eliciting massive immune events for which the cells don’t have the energy to withstand, isn’t the driving force destroying our kids. There’s the epidemic and there are outliers and I’m talking about the epidemic.
The Autism and Bipolar Overlap
Complicating the issue of medicating bipolar kids with antidepressants that cause them to become manic is the fact that the conditions have symptomatic overlap with each other that may result in bipolar kids being given antidepressant medication that is wholly inappropriate for their neurological makeup. Jessica Myszak, PhD, psychologist, told Psych Central that, “Autism and bipolar disorder could both sometimes have sleep difficulties and behaviors that others don’t understand — such as behavioral rigidity, impulsivity, becoming overwhelmed, and differences in speech.“ Additional overlapping symptoms of autism and bipolar disorder could include talking excessively or rapidly, increased stimming (repetitive movements or noises) or fidgeting, impulsivity, aggression, irritability, increased sensitivity to sensory input, difficulties with sleep, self-injurious behaviors, difficulty thinking or concentrating, and suicidal ideation.
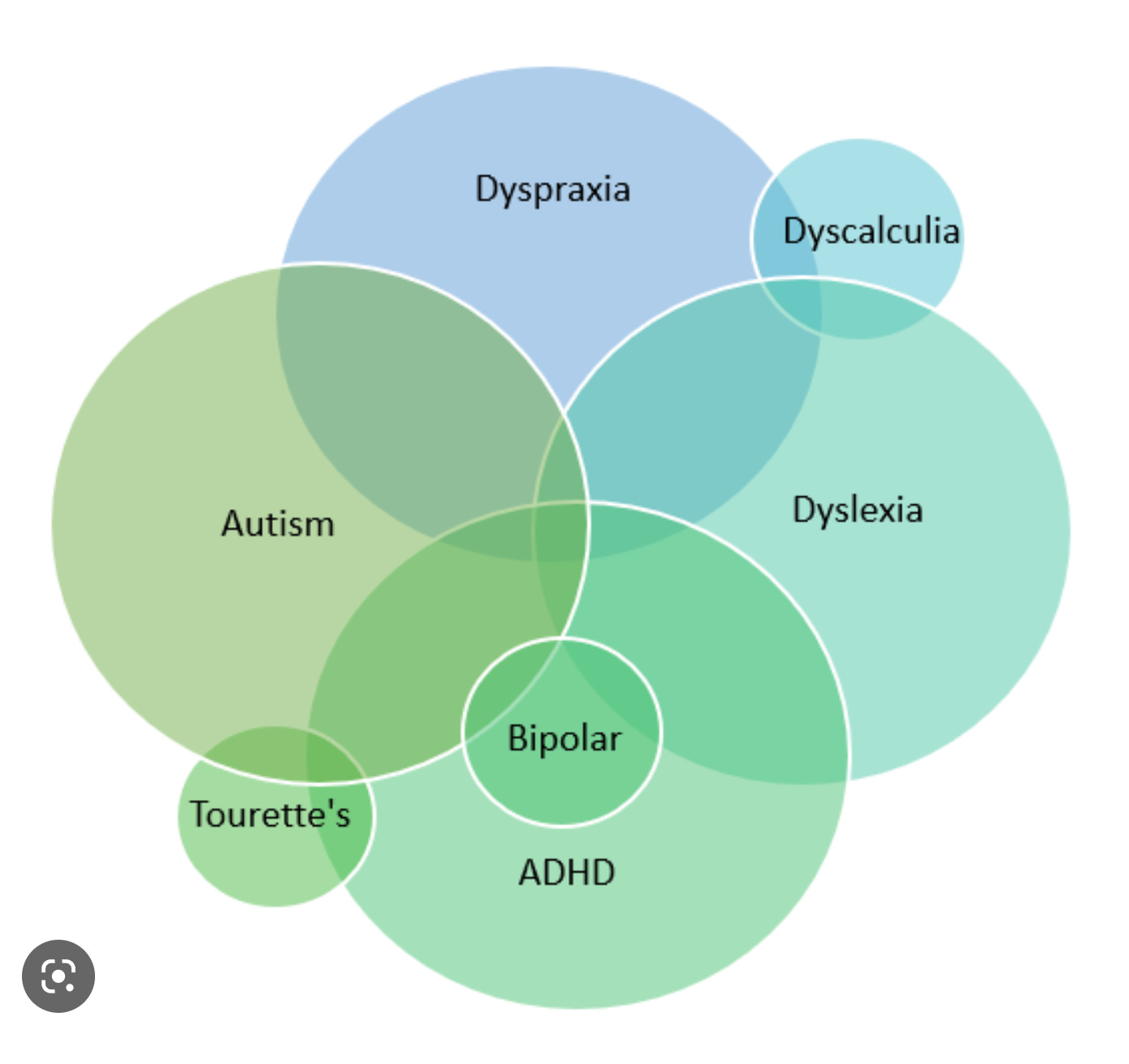
Bipolar disorder seems to sit squarely within an ADHD diagnosis, which many people with high functioning autism have, whether or not they’ve received a formal autism diagnosis. And a small percentage of people with the autism diagnosis overlap with the bipolar diagnosis.
Let’s be serious. How is a pediatrician, or even a psychiatrist, supposed to look at disorders that are entirely based on behavioral symptoms, with no diagnostic tests, and make the right decision about psychotropic drug prescriptions? It’s a guessing game.
Classic Autism vs High Functioning Autism
The term “autism” is derived from the Greek word “autos,” meaning “self, same, spontaneous; directed from within.” In the 1950s, the word “autism” referred to excessive hallucinations and fantasy in infants. However, Michael Rutter, a leading child-psychiatric researcher from the UK’s Maudsley Hospital who conducted the first-ever genetic study of autism, claimed in 1972 that “the autistic child has a deficiency of fantasy rather than an excess.” Rather rapidly, the word “autism” went from describing someone who fantasized excessively to one who did not fantasize at all.
It’s necessary that we make the distinction between classic autism and the high-functioning autism label that was called Asperger’s Syndrome up until recently, when it was thrown under the DSM-5 autism umbrella in order to confuse and dilute the traumatic brain, gut, neurological, and immune system dysfunction knocking our kids out for their entire lives. In my reading of the 85-year history of the symptoms of autism, it seems like classic autism and Asperger’s have been lumped together from the beginning, leading to the idea that the conditions are two wings of the same bird. But the more we learn, the less there seems to be a spectrum tying these two conditions together.
Kids with what was called Asperger’s often exhibit poor social interactions, obsessions, odd speech patterns, limited facial expressions and peculiar mannerisms. They have trouble taking turns during conversations because they want to talk about what they love to talk about without recognizing what others consider to be social norms. They often can’t interpret nonverbal communication like body language and facial expressions. They struggle to empathize with people or feel sympathy for others. They might struggle with emotional regulation. They often can’t understand anyone else’s perspective. Online, we see these kids and young adults discussing how they are entitled use any means necessary to make themselves feel understood. They are, outwardly, the “autos” of autism.
The classic autism kids might come across to outside observers as if there is no one there inside them. Many don’t speak at all. They don’t acknowledge hearing their name. They have severe fine and sometimes gross motor skill impairment, bowel disease, and multiple food allergies. But the classic autism kids who are now mastering Spelling-to Communicate are proving not to be self-obsessed at all. They don’t live in a fantasy world, and they aren’t singularly focused on subjects only they find interesting. They are painfully empathetic. They know every detail of their families’ lives. Once they’re able to communicate, they’re connecting with their parents and siblings, writing poems and senior theses, and announcing they want to go to college. They aren’t scolding their parents for failing to affirm that they were born into the wrong body, insisting on pronoun changes, hormonal injections, or societal buy-in for an identity disorder.
Both sets of kids might show aggression when feeling misunderstood, they’re both likely sensitive to startling or loud sounds, and they both might self sooth with repetitive movements, rocking or spinning. But apart from those sensitive nervous system characteristics, these kids have little in common. One doesn’t graduate from classic autism to high functioning autism with therapy.
I believe that all autism is brain injury, but the DSM-5 did a disservice to every injured child when it lumped them together. It’s now used to deny desperately-needed social therapies for higher-functioning kids who don’t qualify as being “severe enough,” and it watered down the public’s understanding of classic autism and the bodily devastation those kids suffer from. No one would ever say, “I’d rather have an autistic kid than one with measles” if they knew just how bad autism can be.
If Autism Has Been Around Forever, Must It Be Genetic?
The most famous early clinical descriptions of Asperger’s Syndrome (now called high-functioning autism) and classic autism were grouped together and published in The Nervous Child in 1943 by Austrian-American psychiatrist Leo Kanner of Johns Hopkins University. In “Autistic Disturbances of Affective Contact,” Kanner presented eleven case studies of children he had seen since 1938—eight boys and three girls. “These children, who were mesmerized by objects but indifferent to people, had feeding difficulties in infancy, reacted fearfully to loud sounds, and preferred rigid, repetitive routine over any kind of novelty,” he wrote. They engaged in rhythmic spinning, jumping, rolling, and other unusual movements.
Some of the children had no language at all, some had echolalia, repeating the last words said to them. Some of the children were developing normally, then suddenly experienced dramatic regression. Kanner felt that all of them were at normal or above normal intelligence. Almost all of Kanner’s subjects had two parents who were college graduates. One child’s prominent forehead was noted, as were his ragged and enlarged tonsils. A second had enlarged tonsils and adenoids and Kanner wrote that he had reacted to smallpox vaccination at 12 months old. A third child had his tonsils removed, presumably because they were enlarged. Several of them were very poor nursers as infants and vomited frequently. One had a grandfather with OCD behaviors. Most interestingly, many of them had repeated follow-ups where Kanner noted how much the children improved as they aged. You can read the original piece here, if you’d like to.
Even before Kanner’s 1943 paper was published, Austrian psychiatrist Hans Asperger, in 1938, first designated a group of over 200 boys with what is now known as Asperger’s syndrome, but was then called “autistic psychopathy,” meaning autism (self) and psychopathy (personality). The traits Asperger described while observing these children included “a lack of empathy, little ability to form friendships, one-sided conversation, intense absorption in a special interest, and clumsy movements.” Asperger called children with autistic psychopathy “Little Professors,” because of their ability to talk about their favorite subject in great detail.
Should we shrug our shoulders and waive this off with a “Eh, this was way back in 1938, it must be genetic!” It can’t be related to heavy metal toxicity or vaccination if it’s been around that long, right? Or do we dig a little deeper and discover that, beginning in 1932, American and western European parents—the ones who trusted the medical establishment—were repeatedly injecting their infants and children with a brand new mercury and neurotoxic aluminum-containing diphtheria vaccine. The metal doses doubled when tetanus toxoid was added to the vaccine in 1939, and tripled with pertussis in 1942.
Everyone’s Favorite Metal: Mercury
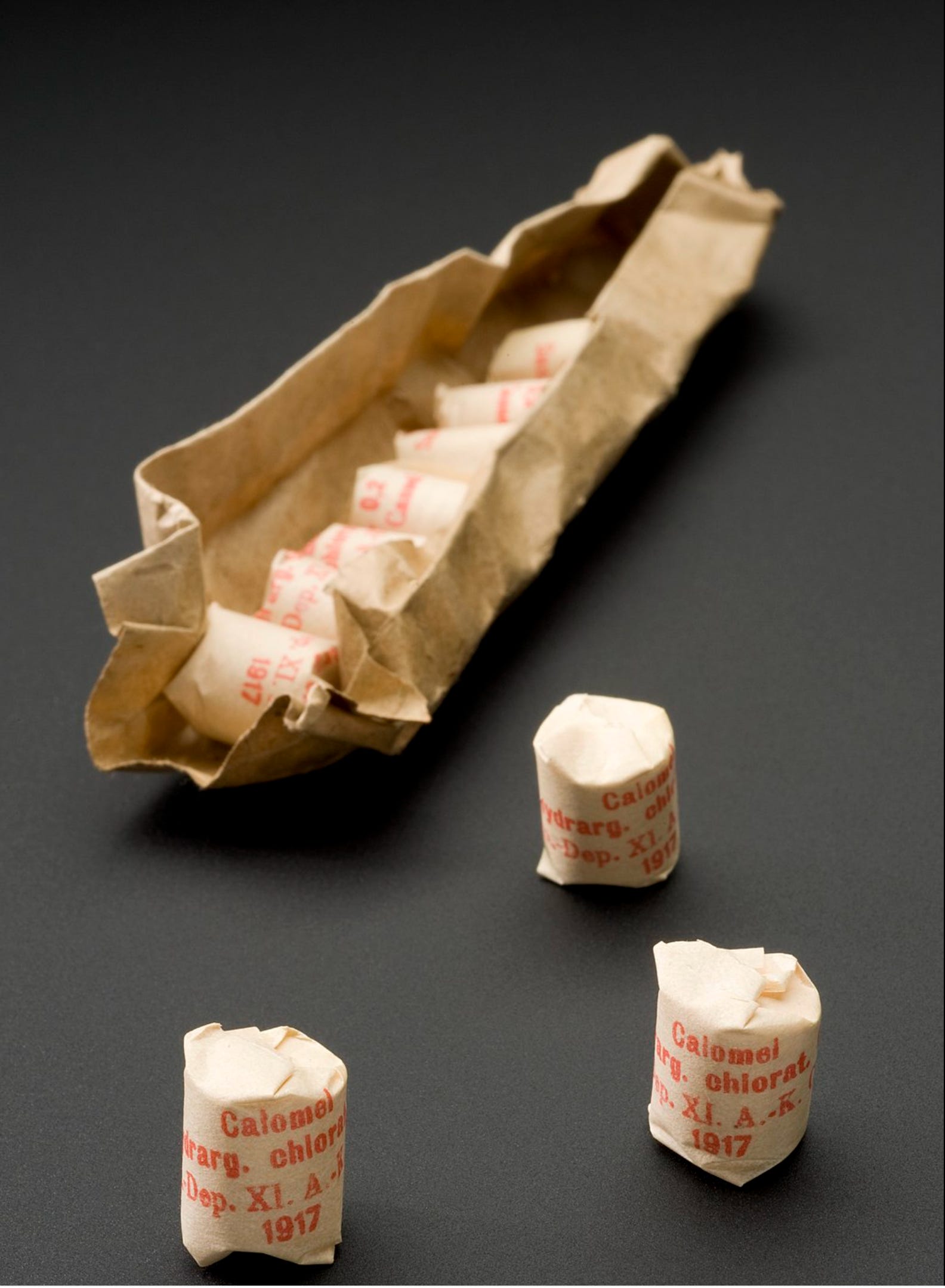
Keep in mind that toxic heavy metal exposures wouldn’t have been limited to vaccination. Anyone who could afford to go to the doctor would have been prescribed mercury, one of the most toxic substances on Earth, as a miracle drug for any number of ailments, sold in the form of calomel, sublimate, cinnober, and oxides of mercury. While calomel was used sparingly throughout the 1700s and early 1800s, by 1840 it was given in heroic doses because the larger dose was believed to be “gentlest on the stomach and bowel.” That was because it caused the bowels to be evacuated immediately rather than be irritated for long periods of time. Medical books of the day taught that, due to the higher temperature in fevered children, kids could withstand even higher calomel doses than adults.
Mercury is well known to cross the placenta and accumulate in fetal tissues. The children in Kanner’s study were all born between 1931 and 1938, when mercury was still used as medicine. What are the odds that their college-educated mothers, who were presumably also born to affluent families with access to medical care, were treated with mercury at some point in their lives? Or even during pregnancy? For how many generations is the mercury passed through the placenta from mother to child?
Something I noticed right away, and that I have never seen discussed anywhere, is the disturbing number of autistic kids in Dr. Kanner’s study born to fathers who were psychiatrists. There were only 11 kids, but Case 5, Case 6, Case 7, and Case 10 were all children of psychiatrists. What are the odds of that? Case 7’s mother was also an MD, and a thoughtful commenter shared with me that she was one of seven physicians who pioneered the numerous “well baby” vaccination visits we’re all subjected to today.
I’ll remind you, just in case you don’t know: one must be an MD to be a psychiatrist. Some other fathers in the study were lawyers and chemists, and all but two of the mothers were college graduates in a time when less than 10% of women graduated from college. Likewise, Dr. Asperger also noted that his “Little Professors” were only found in wealthy, educated families.
{As an entertaining side note, even in the 1930s, psychiatry was regarded as a derelict career; a field chosen when a young doctor couldn’t succeed in any other field of medicine.}
Unfortunately, Kanner didn’t inquire about “medicines” taken in the lifetimes of his patients’ mothers, so we’ll never know what role mercury or vaccines might have played in their children’s outcomes. But more than a third of the Kanner study fathers were doctors with knowledge and access not only to mercury cures and vaccines, but they got their hands on the first psychiatric sedative drugs in existence, like barbiturates and lithium. What better cure to give a doctor’s wife to soothe her anxious nerves? If you’re wondering, yes, barbiturates were certainly abused in the 1930s, with many people taking excessive doses to get high and routinely mixing them with alcohol. Now, modern medicine knows that barbiturates may have teratogenic effects (an agent that causes abnormality following fetal exposure during pregnancy), and many drugs that are teratogenic may give rise to developmental disabilities, autism included.
The Role of the Brain
Asperger’s, or high functioning autism, symptoms include what is likely injuries to the anterior insular cortex area of the brain that controls romantic love, fear, anger, sadness, happiness, empathy, and a “state of union with God.” The syndrome is clearly linked with injury to the angular gyrus in the parietal lobe that is critical to distinguishing left from right; a task that is tricky or impossible for many people with Asperger’s. Unlike classic autism, people with Asperger’s are notoriously ego-centric, and while it’s human tendency for all of us to be ego-centric, we rely on the supramarginal gyrus area of our brains to correct for that—unless it’s injured. Symptoms of Body Integrity Identity Disorder parallel somatoparaphrenia, which happens with damage to the right parietal lobe. Likewise, Body Dysmorphic Disorder probably results from a combination of dysfunctions in frontal-subcortical circuits, temporal, parietal, and limbic structures.
There is no history of “high functioning autism” outside of the history of mercury as medicine, vaccination, and women taking drugs that impact the babies they carry down the road. And there is no denying that autism and gender dysphoria are inextricably linked, probably even more so than we know today, given how many girls have slipped through the cracks of diagnosis. There are no approved drugs for any of autism’s core features, yet 15% of people with high functioning autism are on antidepressants, 7% are on stimulants, 9% are on antipsychotics, and 14% are on hypnotics. And I doubt there is one single school shooter in the last three decades who wasn’t on psychotropic prescriptions from our legal, white coat drug dealers.
And this all came to a head at 10:10 AM on Monday morning in Nashville, Tennessee.
With all of the above in mind, someone please tell me why in the world our nation’s doctors are treating an identity disorder in high functioning autistic kids with chemical castration and surgical mutilation? Looking at it this way, aren’t those services on par with offering up a lobotomy as a solution? Don’t you think kids and young adults suffering from gender dysphoria deserve better than this? Even if your religion forbids this. Even if you are repulsed by it with every fiber of your being. Even if you are flooded with anger and grief over the Tennessee shooting and the Biden Administration’s tone deaf tweets about transgenderism today in light of what just happened. Even if, even if, even if.
Can’t we agree that they deserve better?
LQ
Great read. If you haven’t read it, Dan Olmsted and Mark Blaxill’s book “Age of Autism” is an exhaustive deep dive into the role of mercury in medicine for the last 500 years and how it led to autism. It should have won the Pulitzer Prize. Still should.
You mention the psychiatrists and doctors among Kanner’s children’s parents. Indeed, many psychiatrists treated patients with GPI, an affliction associated with syphilis. Syphilis was treated with mercury at that time. In fact, it was the basis of the famous Tuskegee experiment to withhold it and find out why black men weren’t developing GPI. (Because mercury and syphilis in combination appear to be the cause.)
Most alarming, however, and by far the smoking gun in my opinion, is the mother of one of the original eight Kanner children: Dr. Elizabeth Peabody Trevitt. She is the creator of the well baby visit, quite literally the reason everyone continues to go for “well visits”. She believed a baby couldn’t be vaccinated often or early enough with the new Thimerosal containing diphtheria vaccine in the early 1930’s and is on record saying so. And she is the mother of one of the first children to ever be diagnosed with autism. Think of the tragedy of her legacy? It’s hard to fathom.
Likewise, two of the eight children had fathers who were research professors. They even worked at the same university at one point. (What are the chances of that?) Thimerosal’s sister products were Ceresan and Lignasan, a seed preservative and a lumber preservative respectively. One father was experimenting with Ceresan seeds. They found a brochure for it in his archives during research for their book. The other father was a forestry professor studying Lignasan. Both products were banned by the 80’s for being too toxic. Too toxic for trees. Too toxic for seeds. Still injected into babies and pregnant women.
And then you have child number one, Donald Triplett, who they found first (not those authors of whatever book that was “in a different key” or something like that). He lived in Mississippi, just next to a lumber plant that happened to be one of the first ever to use Lignasan. And his parents just built their first house when he was born.
Oh, and lest we forget that Thimerosal was first used anywhere in the world in two places. Baltimore, Maryland, home of John Hopkins University (where Kanner and the parents in medicine were from including Trevitt) and Austria. (The book explains how this came to be.) We injected babies with mercury in infancy in the US. Austria injected them as toddlers. Both are the birthplaces of autism, classic and Asperger’s.
I could go on. The “coincidences” are innumerable. Mankind has been poisoned by medicine for centuries. The latest manifestations are simply the evidence of how it has evolved. We are here today not only because of that, but also because Leo Kanner made one giant mistake when asking what could be causing it.
It wasn’t that the parents of these children, especially the mothers, were smart or worked, a theory that has led us to this moment. It was what they worked WITH.
And here we are.
Your pieces are always worth the read. Thank you.